
Arsenic
Coliform
Coliform bacteria are organisms that are present in the environment and in the feces of all warm-blooded animals and humans. Coliform bacteria will not likely cause illness. However, their presence in drinking water indicates that disease-causing organisms (pathogens) could be in the water system. Most pathogens that can contaminate water supplies come from the feces of humans or animals.
Role of Coliforms in Detecting Contamination – Testing drinking water for all possible pathogens is complex, time-consuming, and expensive. It is relatively easy and inexpensive to test for coliform bacteria. Total coliform testing is used as an indicator of potential contamination.
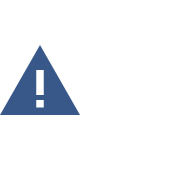
Total Coliform, Fecal Coliform, and E. 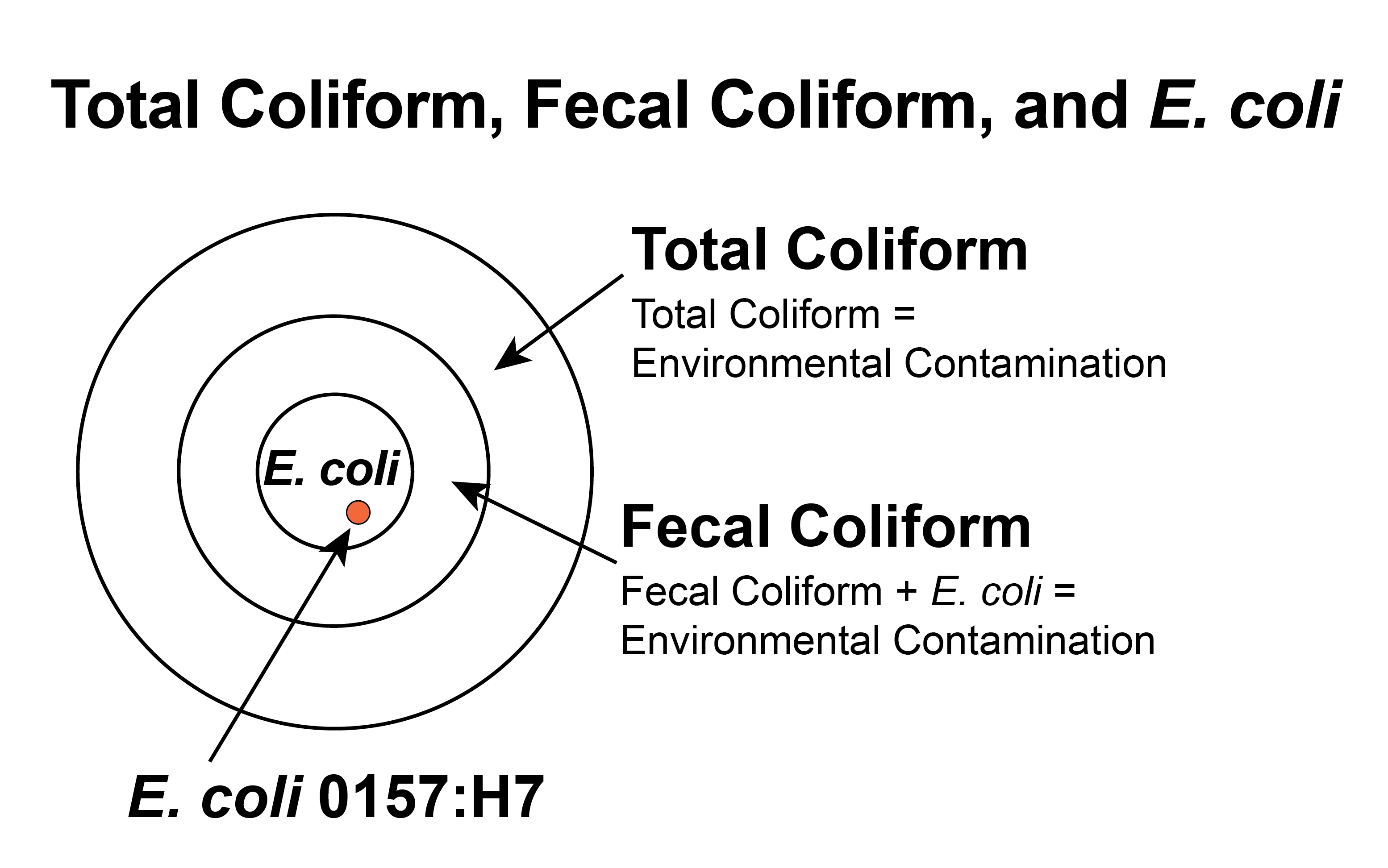 coli – Total coliform bacteria are commonly found in the environment (e.g., soil or vegetation) and are generally not harmful. However, if environmental contamination can enter the system, there may also be a way for pathogens to enter the system.
coli – Total coliform bacteria are commonly found in the environment (e.g., soil or vegetation) and are generally not harmful. However, if environmental contamination can enter the system, there may also be a way for pathogens to enter the system.
Fecal coliform bacteria are a sub-group of total coliform bacteria. They appear in great quantities in the intestines and feces of people and animals. The presence of fecal coliform in a drinking water sample often indicates recent fecal contamination, meaning that there is a greater risk that pathogens are present than if only total coliform bacteria is detected.
E. coli is a sub-group of the fecal coliform group. The presence of E. coli in a drinking water sample almost always indicates recent fecal contamination, meaning there is a greater risk that pathogens are present.
Responses to Coliform Detection – When coliform bacteria are found, water systems investigate to find out how the contamination got into the water. They collect additional, or “repeat,” water samples for testing, and often inspect the entire system. Taking repeat samples helps determine whether an actual problem exists in the system. If any of the repeat samples detect coliform bacteria, the initial findings are considered confirmed. If total coliform bacteria are confirmed in your drinking water, your water system should be inspected to find and eliminate any possible sources of contamination. Once the source is identified, it can usually be resolved by making system repairs, flushing, and adding chlorine for a short period of time.
Confirmation of fecal coliform bacteria or E. coli in a water system indicates recent fecal contamination, which may pose an immediate health risk to anyone consuming the water. Public notification, in the form of a boil advisory or potentially a do not drink advisory, will be issued within 24 hours to alert all water users that there is a health risk associated with the water supply. The notice will inform customers of actions being taken to correct the problem, and when the problem will likely be resolved.
The system will be required to identify the source of contamination, correct the problem, and thoroughly disinfect and flush its system. Once the contamination issue is verified to be resolved the advisory will be lifted.
Health Effects – Symptoms of bacterial waterborne diseases may include gastrointestinal illnesses such as severe diarrhea, nausea, and possibly jaundice as well as minor symptoms like headaches and fatigue. These symptoms are not associated only with disease-causing organisms in drinking water and may be caused by several other factors. Young children and the elderly are usually more susceptible.
Additional Information
Fluoride
Lead
Nitrate
Disinfection Byproducts
Cryptosporidium and Giardia (Surface Water Treatment)
The purpose of the Long Term 2 Enhanced Surface Water Treatment Rule (LT2ESWTR) is to reduce illness linked with the contaminant Cryptosporidium and other microbial pathogens in drinking water. The LT2ESWTR supplements existing regulations for surface water systems, including ground water under the direct influence of surface water (GWUDI) systems, by targeting additional Cryptosporidium treatment requirements for systems with higher risk sources found during LT2ESWTR monitoring. It is important to note that the LT2ESWTR does not require additional Cryptosporidium treatment for all public water systems (PWS). The LT2ESWTR also contains provisions to reduce risks resulting from uncovered finished water reservoirs and to ensure that systems maintain microbial protection as they take steps to decrease the formation of disinfection byproducts that result from chemical water treatment.
Key Provisions
- The LT2ESWTR applies to all PWS supplied by a surface water or GWUDI source.
- All surface water and GWUDI systems must conduct an initial round of source water monitoring and a second round 6 years later for each plant that treats a surface water or GWUDI source. This monitoring includes coli enumeration (and turbidity if required) to determine what level, if any, of additional treatment must be provided.
- Filtered systems must determine their Cryptosporidium treatment bin classification and provide additional treatment for Cryptosporidium, if required.
- All unfiltered systems must provide treatment for Cryptosporidium.
General Source Water Monitoring Information – Any new surface water or GWUDI sources must conduct an initial and a second round of source water monitoring.
Filtered systems serving fewer than 10,000 people must sample their source water (prior to any treatment) for E. coli enumeration (not presence/absence) at least once every two weeks for 12 months.
- Afiltered system serving fewer than 10,000 people may avoid coli monitoring by monitoring for Cryptosporidium and notifying DEQ of this no later than 3 months prior to the date the system is otherwise required to start E. coli monitoring.
- Filtered systems serving fewer than 10,000 people must sample their source water (prior to any treatment) for Cryptosporidium at least twice per month for 12 months or at least monthly for 24 months based on the annual mean coliconcentration of their source water type (lake/reservoir vs. flowing stream).
Systems using GWUDI must also sample their 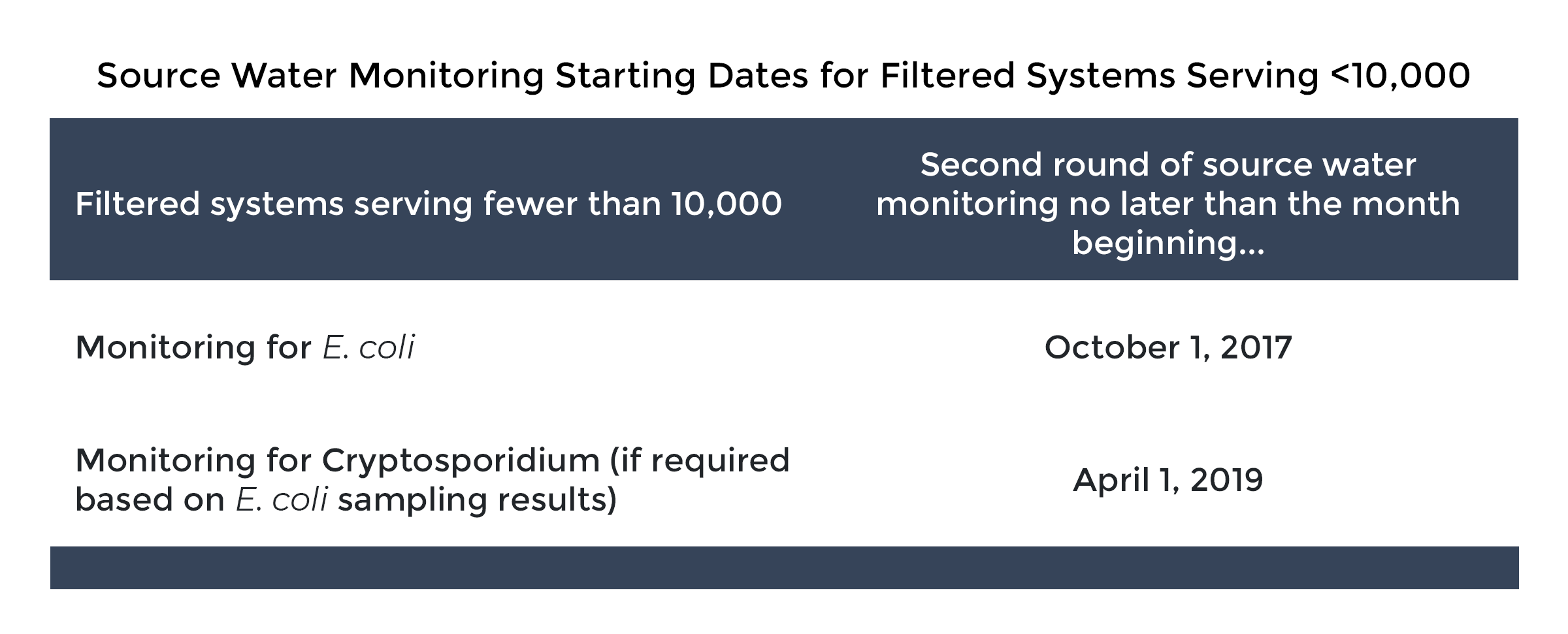 source water (prior to any treatment) for E. coli at least once every two weeks for 12 months based on the E. Coli level that applies to the nearest surface water body. If no surface water body is nearby, the system must comply based on the requirements that apply to systems using lake/reservoir sources.
source water (prior to any treatment) for E. coli at least once every two weeks for 12 months based on the E. Coli level that applies to the nearest surface water body. If no surface water body is nearby, the system must comply based on the requirements that apply to systems using lake/reservoir sources.
Sample Schedule Plans – Prior to sampling, owners and operators must submit to DEQ a sampling plan that includes the following:
- Specific dates for sampling events that must occur at least once every 2 weeks for 12 months for systems serving less than 10,000 people and monitoring for coli, beginning October 1, 2017.
- Samples must be collected within 2 days before or 2 days after the specified date (Wednesdays are recommended), and the results must be submitted to DEQ by the 10th day of the following month.
- Description or diagram of sample location(s) in relation to sources, treatment processes, (including pretreatment), and any filter backwash recycling.
Sample Specific Sampling Requirements – Systems with more than one surface water supply source, one of the following is required for collecting samples:
- Collect samples from a tap where all sources are combined and before any treatment.
- Collect composite samples that represent all sources. In a composite sample, the volume of sample from each source must be weighted according to the proportion of each source in the total plant flow at the time of the sample. You should contact DEQ and your laboratory for assistance.
- Collect and analyze a sample from each source separately and calculate a weighted average of all the results for the sampling date. You should contact DEQ and your laboratory for assistance.
Seasonal Sources
- Owners and operators of systems with seasonal sources need to sample in the months of operation, which is when the plant is running, not only when water is being served.
- If the system operates fewer than 6 months a year, two sampling periods, with six evenly spaced samples in each period, must take place over the course of 2 seasons. For example, if a system operates May through September, they would sample May through September 2017 and again in May – September 2018).
- If the system operates ≥ 6 months but less than a full year, two sampling periods during months of operation must take place and samples must be taken at least once every 2 weeks.
Systems Using Bank Fileration
- Systems using bank filtration followed by a filtration plant must collect samples from the well and after bank filtration.
- Systems receiving Cryptosporidium treatment credit for bank filtration must collect source water samples in the surface water before bank filtration.
If conditions pose a danger to someone collecting samples or are unforeseen and could not be avoided that prevent a sample from being collected, the operator must collect a sample as close to the scheduled date as possible and submit an explanation for the new sampling date along with the laboratory results.
Sample Collection and Submission
- EPA Crypto and Sample Collection Recommendations – Pocket Guide
- EPA LT2ESWTR Source Water Monitoring Guidance
**NOTE – Samples must be maintained at 0–10 oC (32–50 oF), but not frozen, during shipment to the laboratory for E.coli enumeration analysis. Samples received outside this temperature range will be rejected.
Bin Calculation for Filtered Systems – Following the completion of the second round of source water monitoring, DEQ will recalculate each PWS’s Cryptosporidium bin concentration using the results reported.
- Step #1 – The results of all the samples for 12 months (one sample at least every two weeks) are added together.
- Step #2 – The sum of all the samples from Step #1 is divided by the total number of samples to determine the annual mean.
Under LT2ESWTR, DEQ may approve an alternative to the small water system E. coli trigger levels (currently 10 E. coli/100ml for lake/reservoir or less than 50 E.coli/100ml for flowing stream sources.
According to EPA “analysis indicates 100 E. coli/100ml for lake/reservoir AND flowing streams provide more accurate identification of systems requiring Crypto monitoring and compliance with LT2 treatment technique requirements.” Idaho has adopted this approach of using 100 E. coli/100 ml.
Additional Resources
- Acrylamide and Epichlorohydrin Certification Form
- Implementation Guidance for the LT2EWSTR
- LT2ESWTR E.coli Sample Information Required for Lab Analysis from PWS
- Summary of E.coli Enumeration Sampling Collection Under LT2ESWTR
- Idaho Drinking Water Labs Certified for LT2ESWTR
- EPA LT2ESWTR webpage
- EPA LT2ESWTR Source Water Monitoring Guidance
- EPA LT2ESWTR Source Water Monitoring Factsheet for PWSs serving <10,000
- EPA LT2ESWTR Small Entity STEP Guide
- EPA Crypto and coli Sampling Recommendations – Pocket Guide
Cyanotoxins
Cyanobacteria, often referred to as blue-green algae, are bacteria that photosynthesize like algae and plants. Cyanobacteria naturally occur in freshwater environments but, under certain conditions, can reproduce rapidly and form floating mats and dense surface scums, commonly referred to as harmful algae blooms (HABs). HABs produce cyanotoxins, which can pose a risk to human health.
EPA is determining whether to regulate cyanotoxins in drinking water due to updated health information and occurrence data. EPA included several types of cyanotoxins in their fourth Unregulated Contaminant Monitoring Rule (UCMR4), which requires all public water systems utilizing surface water or ground water influenced by surface water and serving over 10,000 customers to monitor for certain cyanotoxins. UCMR4 also applies to some smaller systems.
 Cyanotoxin health advisory levels – In 2015, EPA established health advisory levels for two cyanotoxins: microcystin and cylindrospermopsin. Health advisory levels are recommended contaminant levels meant to provide a margin of protection for all water system users based on a specified exposure time from adverse health effects resulting from the contaminant. When these toxins are found in drinking water, the concentrations should be compared with the health advisory levels.
Cyanotoxin health advisory levels – In 2015, EPA established health advisory levels for two cyanotoxins: microcystin and cylindrospermopsin. Health advisory levels are recommended contaminant levels meant to provide a margin of protection for all water system users based on a specified exposure time from adverse health effects resulting from the contaminant. When these toxins are found in drinking water, the concentrations should be compared with the health advisory levels.
See EPA’s website for health advisory information for cyanotoxins.
Health effects of cyanotoxins – Adverse health effects from cyanotoxins depend on many factors, including the type of cyanotoxin(s) present, duration of exposure, and the age and health of the individual. Cyanotoxins may affect the liver, nervous system, or skin, depending on the toxin. Health effects from cyanotoxin exposure range from skin rashes to liver and nerve damage. No human deaths in the United States have been caused by cyanotoxins, however, pet, livestock, and wildlife deaths caused by cyanotoxins have been reported throughout the United States and the world.
If you concerned about your health or have symptoms, contact your healthcare provider.
Public water systems monitoring for cyanotoxins in Idaho – Public water systems are not required to monitor for cyanotoxins. Some systems may voluntarily monitor for cyanotoxins. Contact your public water system to find out if they monitor for cyanotoxins.
Removing cyanotoxins from water – Boiling water will not remove cyanotoxins and will concentrate the toxins.
If your drinking water has been impacted by cyanotoxins and a “Do Not Use” or a “Do Not Drink” order has been issued, use an alternative source of water for drinking.
Point-of-use devices can be used to reduce levels of microcystins. National Sanitation Foundation International developed NSF Protocol 477: Drinking Water Treatment Units – Microcystin that verifies a water filter’s ability to reduce microcystin below the health advisory levels set by EPA.
Treatment devices require regular maintenance such as changing filters, cleaning scale buildup, or disinfecting the unit. Failure to properly maintain a unit reduces its effectiveness and, in some cases, may further impair the water quality. Follow the manufacturer’s recommendations for replacements and maintenance.
Once a cyanotoxin-related health advisory is lifted, you should flush all of your household plumbing and replace all water filters in the house to remove toxins:
- Run and flush hot water taps for 15 minutes and all cold water taps for 5 minutes.
- Change all filters on point of use units, point of entry systems, refrigerator water filters, and membranes for reverse osmosis units.
- Ensure all faucets and plumbed appliances have been flushed.
- Additional flushing instructions.
Additional Resources